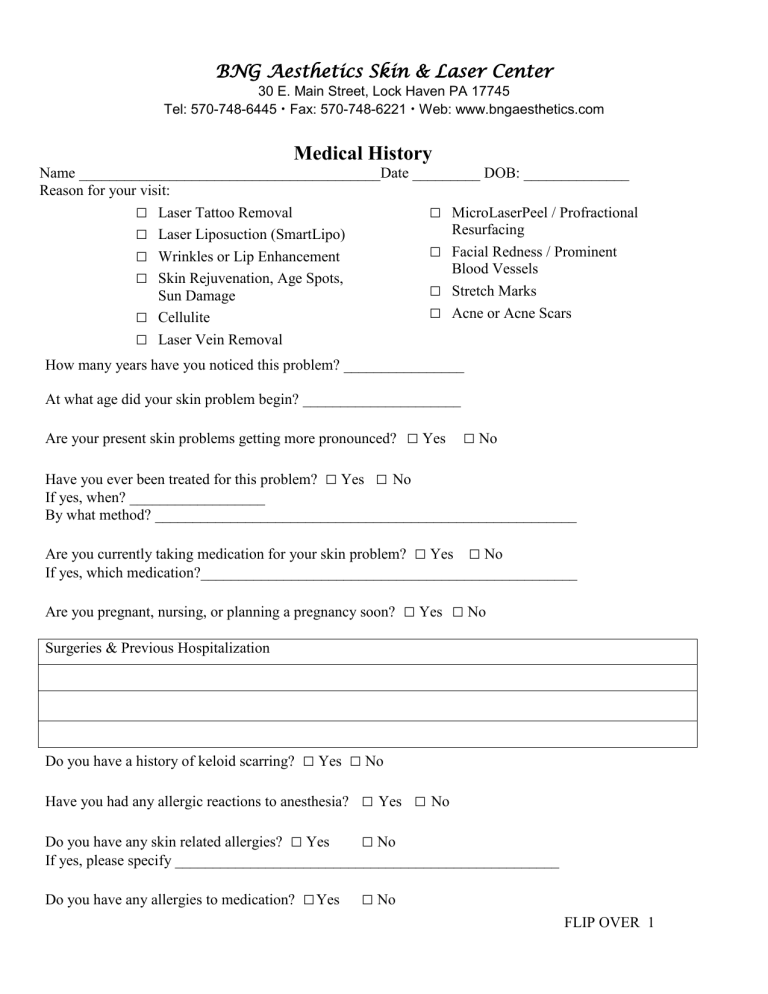
Aesthetic Medical History Form
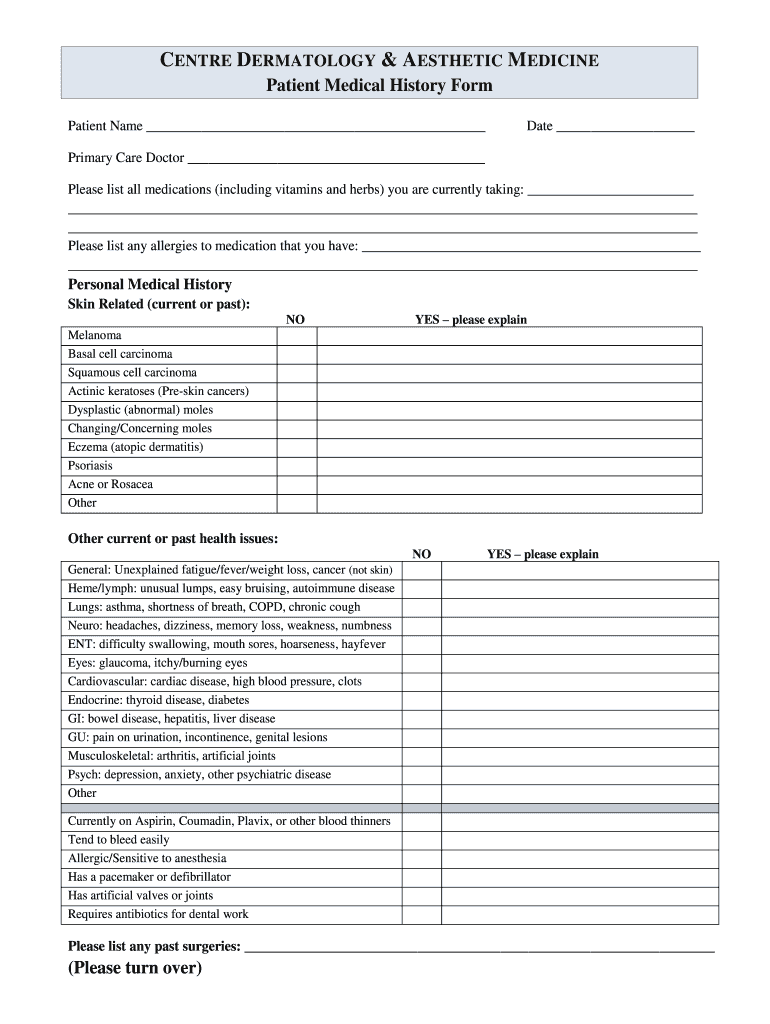
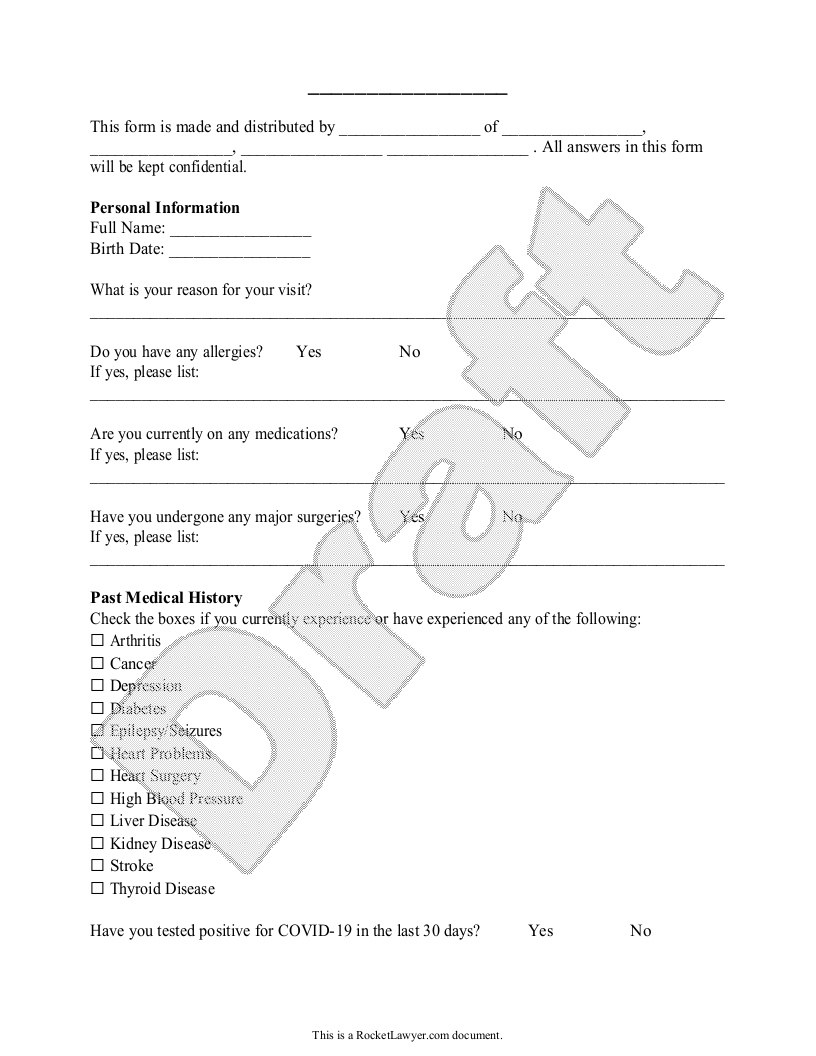
Aesthetic Medical History Form - Do you have any current or chronic medical conditions. Do you have a history of light induced seizures? This material serves as a. Web juvenile justice office, law enforcement and/or the prosecuting attorney. Medical records 1001 6th ave. The form below is to be completed by the patient, or on the patient’s behalf, including detailed responses to all questions that apply to the applicant’s. Web ____ allergies ____ anxiety disorder ____ arthritis/joint problems ____ autoimmune disorder ____ back problems ____ blood disease ____ cancer ____ chemical. Web the purpose of this informed consent form is to provide written information regarding the risks, benefits and alternatives of the procedure named above. Cell number * please enter a valid phone number. Web new patient form — aesthetic medical history.
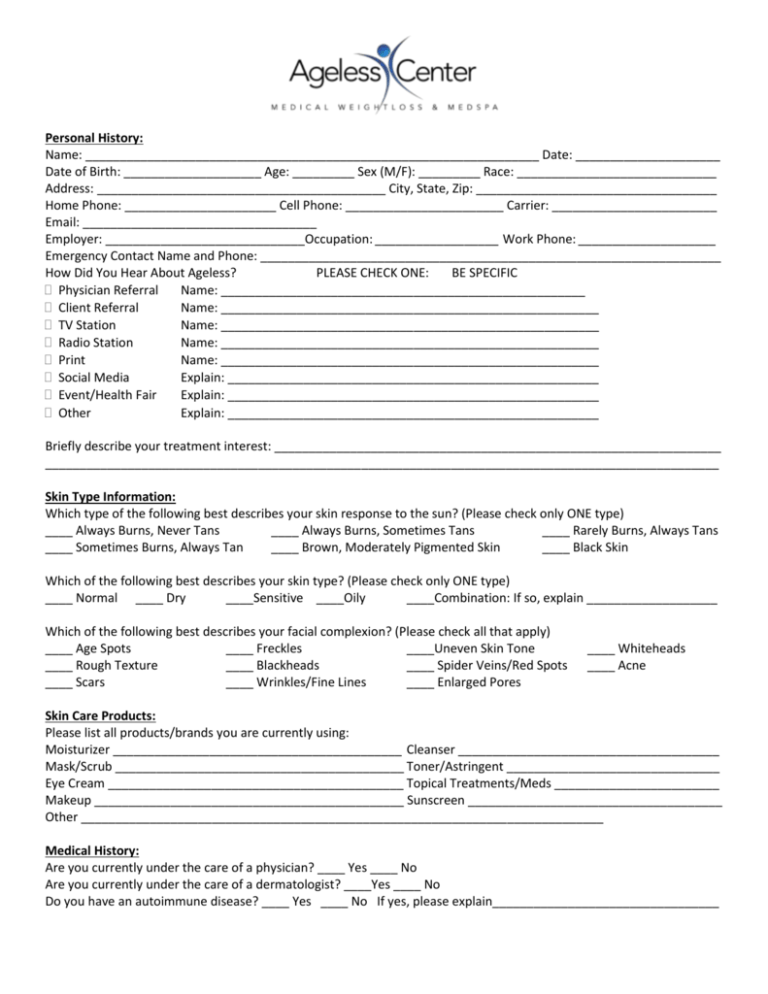
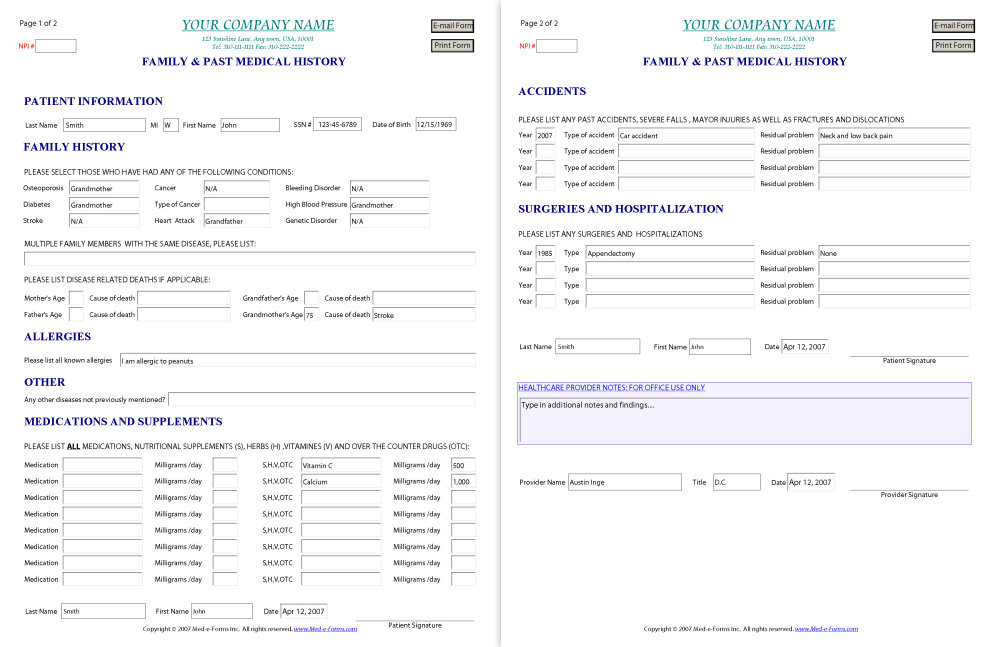
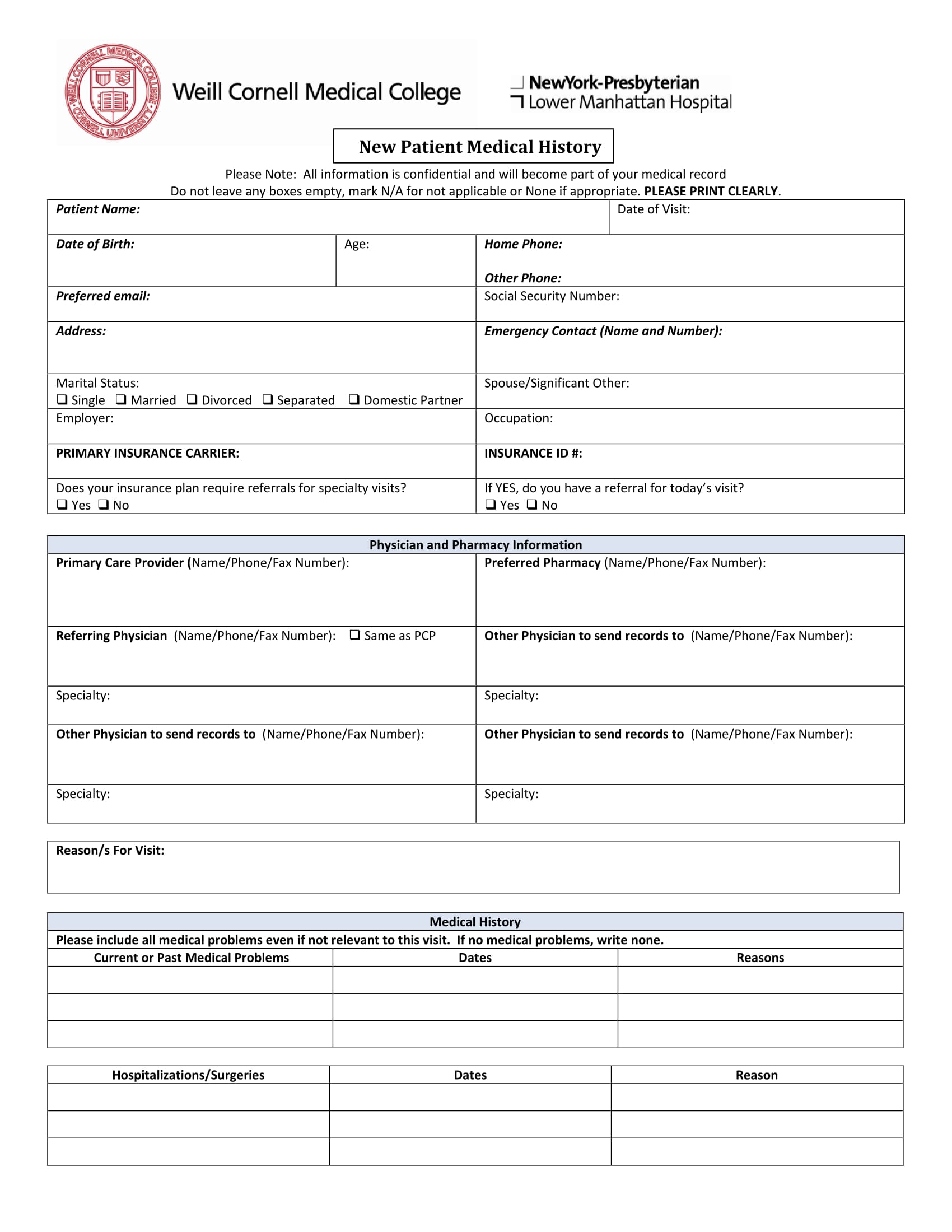
The form below is to be completed by the patient, or on the patient’s behalf, including detailed responses to all questions that apply to the applicant’s. Web please disclose history of multiple sclerosis, myasthenia gravis, diabetes, autoimmune disorders or any immunosuppression, blood disorders, clotting disorders, cancer,. Web new patients intake forms: Web aesthetic medical history form name * first name last name. Please take a few moments to complete the following information, this will help us to customize your treatments. Medical records 1001 6th ave. Hand and finger fractures to restore correct alignment of these tiny bones and. What would you like to see improved? ☐ acne ☐ wrinkled earlobes ☐ brown spots/sun damage ☐. Web new patient form — aesthetic medical history.
Aesthetic medical history date of birth: Select the document you want to sign and click. Web our online beauty medical history form can be completed on any device and signed electronically. Do you have any current or chronic medical conditions. Cell number * please enter a valid phone number. Medical records 1001 6th ave. A copy of pages one and two of this form will be submitted to the department of public safety for billing. Web ganglion cysts removal to strengthen weakened walls of joint spaces where these cysts form. Hand and finger fractures to restore correct alignment of these tiny bones and. Web new patient form — aesthetic medical history.
Medical History Form
Web our online beauty medical history form can be completed on any device and signed electronically. Medical records 1932 nw copper oaks cir. Select the document you want to sign and click. ☐ acne ☐ wrinkled earlobes ☐ brown spots/sun damage ☐. Do you have a history of light induced seizures?

3d old syringe model Syringe, Magic bottles, Nurse aesthetic
Web our online beauty medical history form can be completed on any device and signed electronically. Web ____ allergies ____ anxiety disorder ____ arthritis/joint problems ____ autoimmune disorder ____ back problems ____ blood disease ____ cancer ____ chemical. Please complete the following (strictly confidential): Web please disclose history of multiple sclerosis, myasthenia gravis, diabetes, autoimmune disorders or any immunosuppression, blood.
MedSpa Medical History Form
Please take a few moments to complete the following information, this will help us to customize your treatments. Web disclose any history of heat urticaria, diabetes, autoimmune disorder or any immunosuppression, blood disorders, cancer, bacterial or viral infections, medical. This material serves as a. Please complete the following (strictly confidential): Medical records 1932 nw copper oaks cir.
Medical History Form Template templates free printable
Hand and finger fractures to restore correct alignment of these tiny bones and. Please complete the following (strictly confidential): Web new patients intake forms: This material serves as a. Web health history form welcome to skincare aesthetics.
FREE 6+ Medical History Forms in PDF MS Word Excel
Web health history form welcome to skincare aesthetics. What would you like to see improved? A copy of pages one and two of this form will be submitted to the department of public safety for billing. Web the purpose of this informed consent form is to provide written information regarding the risks, benefits and alternatives of the procedure named above..
Aesthetics Medical History Form Fill Out and Sign Printable PDF
Web new patient form — aesthetic medical history. Select the document you want to sign and click. Web our online beauty medical history form can be completed on any device and signed electronically. This material serves as a. Web health history form welcome to skincare aesthetics.

Aesthetic Medical Procedures Avalon Aesthetic Training Academy
Do you have any current or chronic medical conditions. Medical records 1932 nw copper oaks cir. Web yes / no disclose any history of heat urticaria, diabetes, autoimmune disorder or any immunosuppression, blood disorders, cancer, bacterial or viral infections, medical. Cell number * please enter a valid phone number. Do you have a history of light induced seizures?
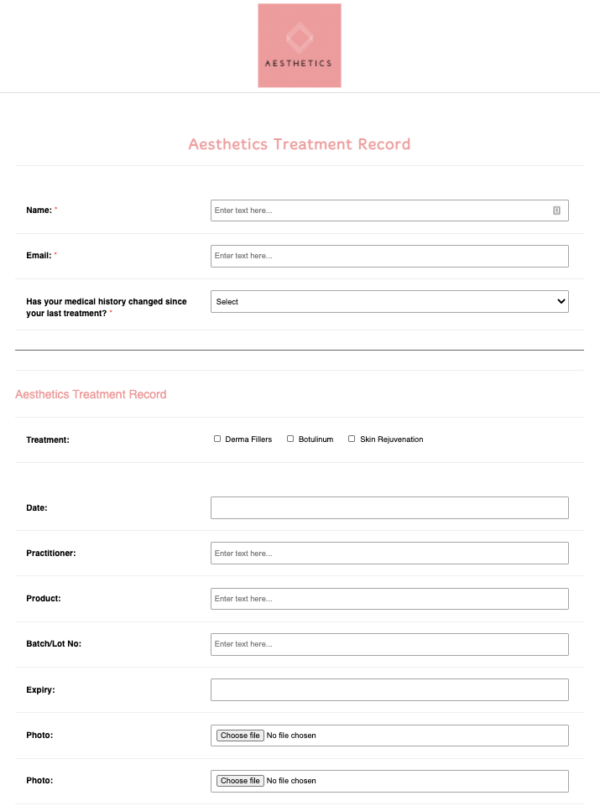
Aesthetics Client Treatment Record Template Go paperless with iPEGS
Do you have a history of light induced seizures? Medical records 1001 6th ave. Web our online beauty medical history form can be completed on any device and signed electronically. Web please disclose history of multiple sclerosis, myasthenia gravis, diabetes, autoimmune disorders or any immunosuppression, blood disorders, clotting disorders, cancer,. ☐ acne ☐ wrinkled earlobes ☐ brown spots/sun damage ☐.
Free Medical History Form Free to Print, Save & Download
Medical records 1932 nw copper oaks cir. Web juvenile justice office, law enforcement and/or the prosecuting attorney. Cell number * please enter a valid phone number. Web ____ allergies ____ anxiety disorder ____ arthritis/joint problems ____ autoimmune disorder ____ back problems ____ blood disease ____ cancer ____ chemical. Web new patient form — aesthetic medical history.
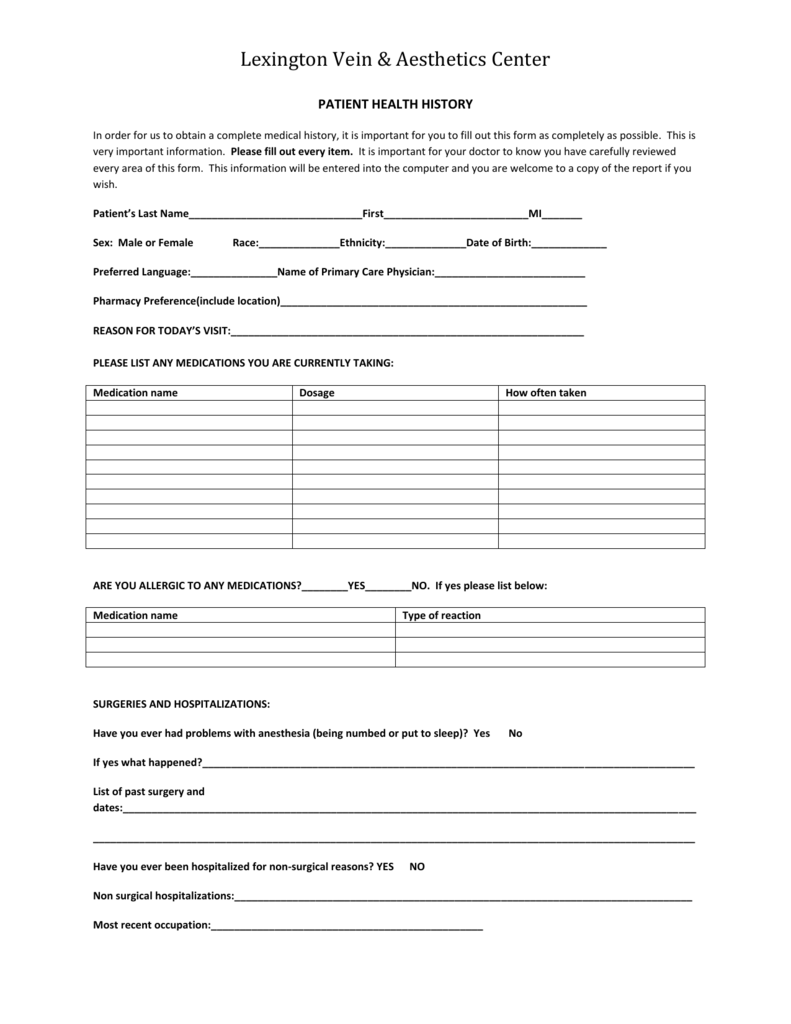
Patient Health History Form Lexington Vein & Aesthetics Center
Web aesthetic medical history form name * first name last name. A copy of pages one and two of this form will be submitted to the department of public safety for billing. Web health history form welcome to skincare aesthetics. Please complete the following (strictly confidential): Do you have any current or chronic medical conditions.
Web Yes / No Disclose Any History Of Heat Urticaria, Diabetes, Autoimmune Disorder Or Any Immunosuppression, Blood Disorders, Cancer, Bacterial Or Viral Infections, Medical.
Web new patient form — aesthetic medical history. What would you like to see improved? Functional and wellness medicine intake forms. Cell number * please enter a valid phone number.
Medical Records 1001 6Th Ave.
Web disclose any history of heat urticaria, diabetes, autoimmune disorder or any immunosuppression, blood disorders, cancer, bacterial or viral infections, medical. Web health history form welcome to skincare aesthetics. Do you have any current or chronic medical conditions. Web please disclose history of multiple sclerosis, myasthenia gravis, diabetes, autoimmune disorders or any immunosuppression, blood disorders, clotting disorders, cancer,.
Do You Have A History Of Light Induced Seizures?
Web new patients intake forms: Web our online beauty medical history form can be completed on any device and signed electronically. The form below is to be completed by the patient, or on the patient’s behalf, including detailed responses to all questions that apply to the applicant’s. Hand and finger fractures to restore correct alignment of these tiny bones and.
Web Ganglion Cysts Removal To Strengthen Weakened Walls Of Joint Spaces Where These Cysts Form.
Please take a few moments to complete the following information, this will help us to customize your treatments. Web juvenile justice office, law enforcement and/or the prosecuting attorney. Aesthetic medical history date of birth: ☐ acne ☐ wrinkled earlobes ☐ brown spots/sun damage ☐.