Blue Cross Dispute Form
Blue Cross Dispute Form - Web submission of this form constitutes agreement not to bill the patient during the dispute process. Fields with an asterisk (*) are required. Web blue cross blue shield of arizona. Use this form to select an individual or entity to act on your behalf during the disputed claims process. If you receive services outside capital. If coverage or payment for an item or medical service is denied that you think should be covered. To prevent any delay in the review process, please ensure the form is filled out completely, signed and dated, and included with the dispute request. Box 13466, mail stop a116. This form must be included with your request to ensure that it is routed to the appropriate area of the. Web if you have a problem with your blue cross blue shield of michigan service, you can use this form to file an appeal with us.
Carefirst bluechoice must receive your written appeal within 180 days of the date of notification of the denial of benefits or services. A) pay the claim or b) write to you and maintain our denial or c) ask you. Save or instantly send your ready documents. By mail or by fax:. This form must be included with your request to ensure that it is routed to the appropriate area of the. Web blue cross' medicare advantage ppo providers should follow the guidelines on this page when submitting an appeal. Web blue cross blue shield of arizona. Box 13466, mail stop a116. Web filing a medical appeal appeals: Michigan providers can either call or write to make an appeal.
• request an appeal if you feel we didn’t cover or pay enough for a service or drug you received. Which form to use and when if you are a provider who is contracted to provide care and services to our blue cross community health plans. Web blue cross blue shield of arizona. Michigan providers can either call or write to make an appeal. Before submitting a pricing dispute, we require you to. Medicaid claims inquiry or dispute request form. Web complete capital blue cross provider dispute form online with us legal forms. Web filing a medical appeal appeals: Medical appeals and grievances department. By mail or by fax:.
2022 Credit Dispute Form Fillable, Printable PDF & Forms Handypdf
Web submission of this form constitutes agreement not to bill the patient during the dispute process. Web complete capital blue cross provider dispute form online with us legal forms. If you're a blue cross blue shield of michigan. If you receive services outside capital. Web appeal and grievance form appeal or grievance?
Fifththird Com Form Fill Out and Sign Printable PDF Template signNow
Before submitting a pricing dispute, we require you to. Web appeal and grievance form appeal or grievance? Medical appeals and grievances department. By mail or by fax:. Carefirst bluechoice must receive your written appeal within 180 days of the date of notification of the denial of benefits or services.
Toll Dispute Form Fill Out and Sign Printable PDF Template signNow
Medical appeals and grievances department. Web complete capital blue cross provider dispute form online with us legal forms. Please complete the form below. • request an appeal if you feel we didn’t cover or pay enough for a service or drug you received. Medicaid claims inquiry or dispute request form.

Dispute Crystal Blue Hexagon Button Stock Illustration Illustration
Medicaid claims inquiry or dispute request form. Use the pricing dispute form (below) to disagree with the contractual pricing of a claim or claim line. Box 13466, mail stop a116. If you're a blue cross blue shield of michigan. Michigan providers can either call or write to make an appeal.
Equifax Dispute Form Fill Out and Sign Printable PDF Template signNow
Web medicaid dispute request forms: Medical appeals and grievances department. You can ask for an appeal if coverage or payment for an item or medical service is denied that you think should be covered. By mail or by fax:. Use this form to select an individual or entity to act on your behalf during the disputed claims process.
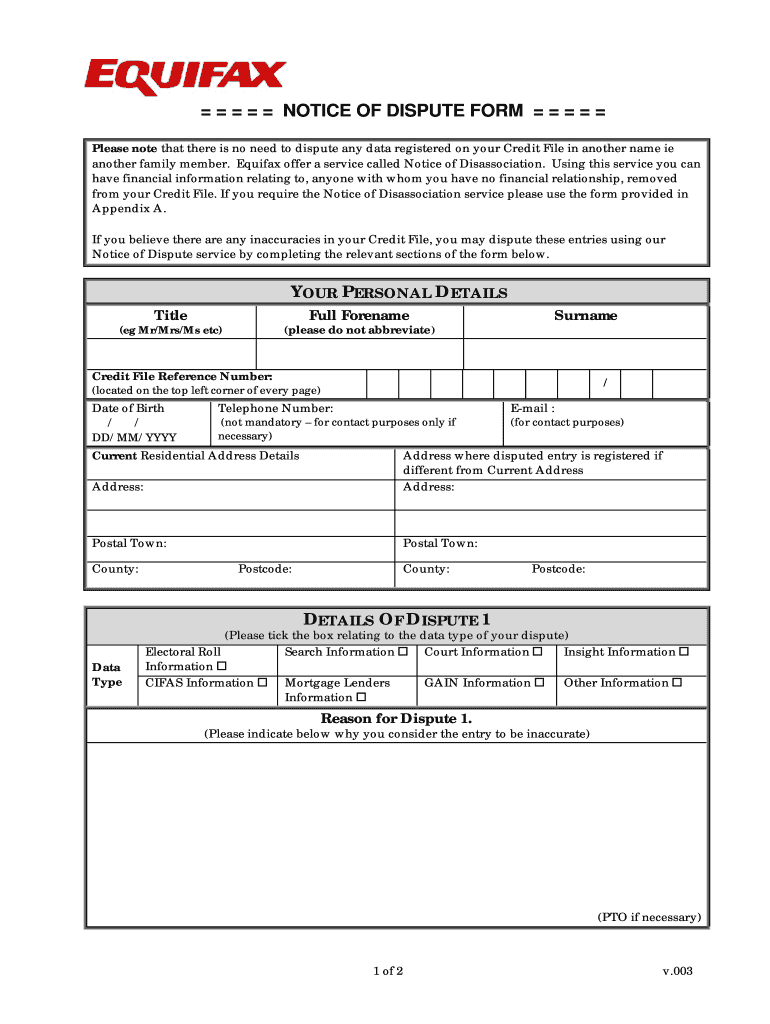
Equifax Dispute Form Fill Out and Sign Printable PDF Template signNow
Web appeal and grievance form appeal or grievance? Web blue cross blue shield of arizona. Use the pricing dispute form (below) to disagree with the contractual pricing of a claim or claim line. Box 13466, mail stop a116. Save or instantly send your ready documents.

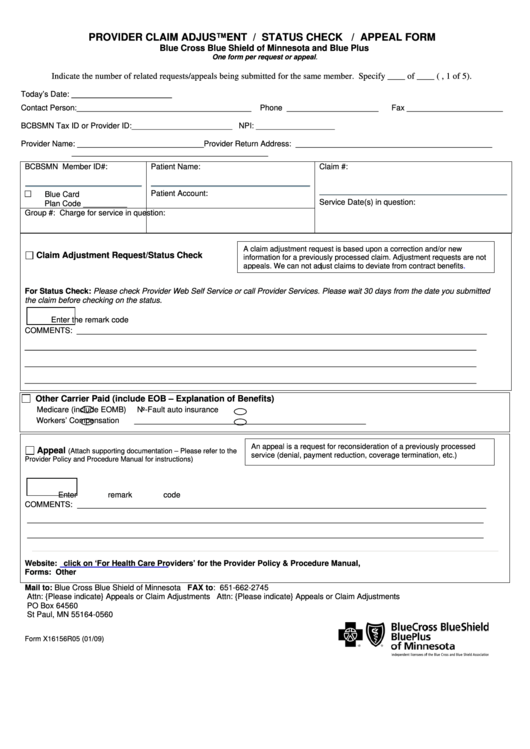
BCBS in Provider Dispute Resolution Request Form PDF Blue Cross
Web appeal and grievance form appeal or grievance? To prevent any delay in the review process, please ensure the form is filled out completely, signed and dated, and included with the dispute request. Carefirst bluechoice must receive your written appeal within 180 days of the date of notification of the denial of benefits or services. • request an appeal if.
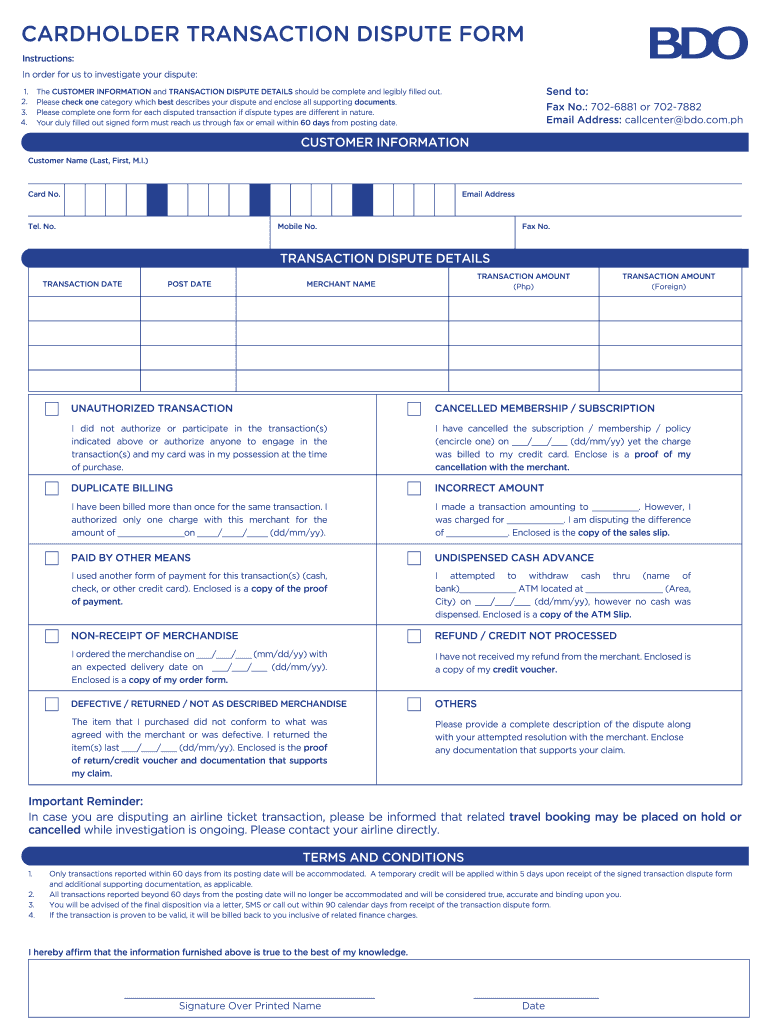
Bdo Dispute Form Fill Online, Printable, Fillable, Blank pdfFiller
Web blue cross' medicare advantage ppo providers should follow the guidelines on this page when submitting an appeal. If coverage or payment for an item or medical service is denied that you think should be covered. If you're a blue cross blue shield of michigan. This form must be included with your request to ensure that it is routed to.
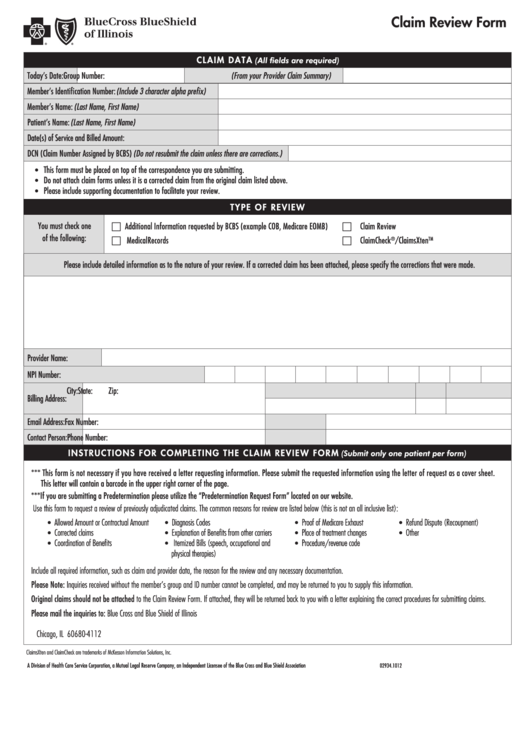
Fillable Claim Review Form Blue Cross And Blue Shield Of Texas
You can ask for an appeal: Web this form is for all providers requesting information about claims status or disputing a claim with blue cross and blue shield of illinois (bcbsil) and serving members in the state. Easily fill out pdf blank, edit, and sign them. Medical appeals and grievances department. Use the pricing dispute form (below) to disagree with.
Blue Cross Blue Shield Coverage Check change comin
Web complete capital blue cross provider dispute form online with us legal forms. If you're a blue cross blue shield of michigan. Web this form is for all providers requesting information about claims status or disputing a claim with blue cross and blue shield of illinois (bcbsil) and serving members in the state. Web medicaid dispute request forms: Save or.
Use The Pricing Dispute Form (Below) To Disagree With The Contractual Pricing Of A Claim Or Claim Line.
Web complete capital blue cross provider dispute form online with us legal forms. If you receive services outside capital. Web provider dispute form complete this form to file a provider dispute. • request an appeal if you feel we didn’t cover or pay enough for a service or drug you received.
If You're A Blue Cross Blue Shield Of Michigan.
You can ask for an appeal: Medicaid claims inquiry or dispute request form. Web filing a medical appeal appeals: Web blue cross blue shield of arizona.
Web Authorized Representative Designation Form.
Before submitting a pricing dispute, we require you to. You can ask for an appeal if coverage or payment for an item or medical service is denied that you think should be covered. Easily fill out pdf blank, edit, and sign them. Each claim review form must include the.
By Mail Or By Fax:.
If coverage or payment for an item or medical service is denied that you think should be covered. Which form to use and when if you are a provider who is contracted to provide care and services to our blue cross community health plans. Please complete the form below. Medical appeals and grievances department.