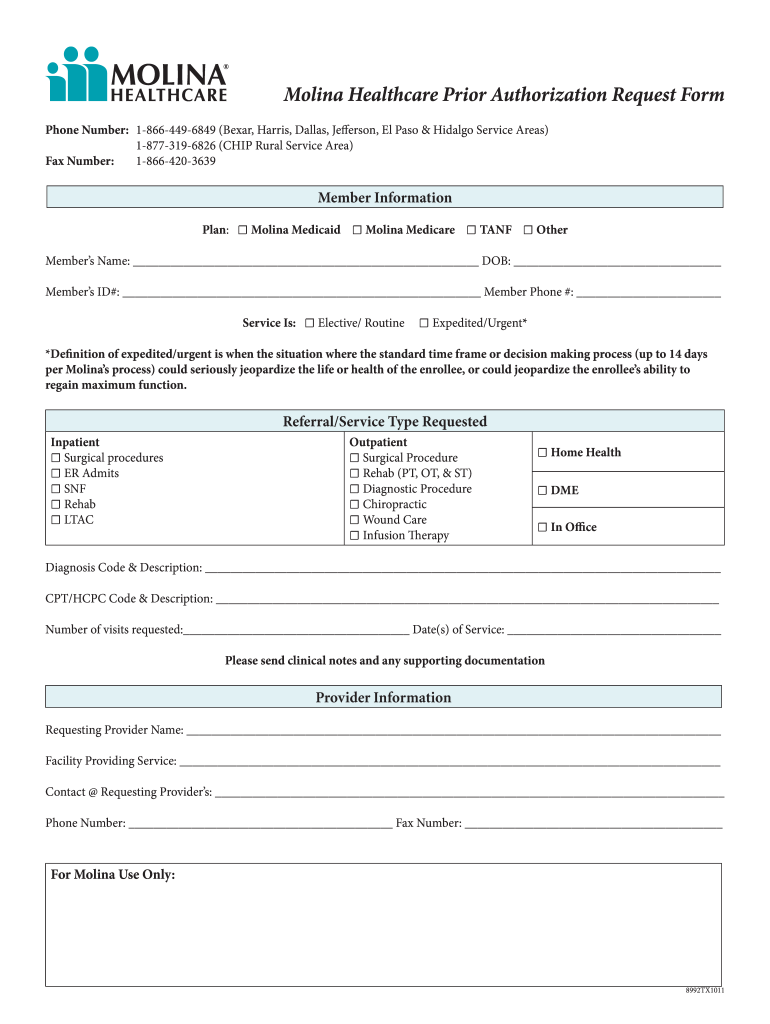
Molina Referral Form
Molina Referral Form - Web if you would like to appoint a representative, you and your appointed representative must complete this form and mail it to molina dual options at: Cs day habilitation programs referral form. 01/01/18) pregnancy notification form frequently used forms claims announcements. Cs medically tailored meals referral form. This referral is valid for 90 days or up to 6 months only. Cs personal care and homemaker services referral form. Odm health insurance fact request form. Request for external wheelchair assessment form. Cs recuperative care referral form. Molina healthcare of california 200 oceangate, suite 100 long beach, ca 90802
Cs personal care and homemaker services referral form. Referral or prior authorization is needed Request for external wheelchair assessment form. Cs medically tailored meals referral form. Cs day habilitation programs referral form. Web critical incident referral template (medicaid only) ohio urine drug screen prior authorization (pa) request form. This referral is valid for 90 days or up to 6 months only. Cs recuperative care referral form. Web if you would like to appoint a representative, you and your appointed representative must complete this form and mail it to molina dual options at: 2023 medicaid pa guide/request form (vendors).
Web molina healthcare of washington, inc. Referral or prior authorization is needed Web critical incident referral template (medicaid only) ohio urine drug screen prior authorization (pa) request form. Cs recuperative care referral form. Critical incident form email comped et l form o:t [email protected] type of incident (required by aso/mcos) ☐ severely adverse medical outcome or death occurring within 72 hours of transfer from a contracted behavioral facility to a medical treatment facility Molina healthcare of california 200 oceangate, suite 100 long beach, ca 90802 2023 medicaid pa guide/request form (vendors). Cs day habilitation programs referral form. This referral is valid for 90 days or up to 6 months only. 01/01/18) pregnancy notification form frequently used forms claims announcements.
Molina prior authorization form Fill out & sign online DocHub
Odm health insurance fact request form. Web molina healthcare of washington, inc. Cs day habilitation programs referral form. Cs medically tailored meals referral form. Molina healthcare of california 200 oceangate, suite 100 long beach, ca 90802

MOLINA HEALTHCARE, INC. FORM 8K EX99.1 September 16, 2011
Cs day habilitation programs referral form. Web if you would like to appoint a representative, you and your appointed representative must complete this form and mail it to molina dual options at: Referral or prior authorization is needed Odm health insurance fact request form. Web molina healthcare of washington, inc.
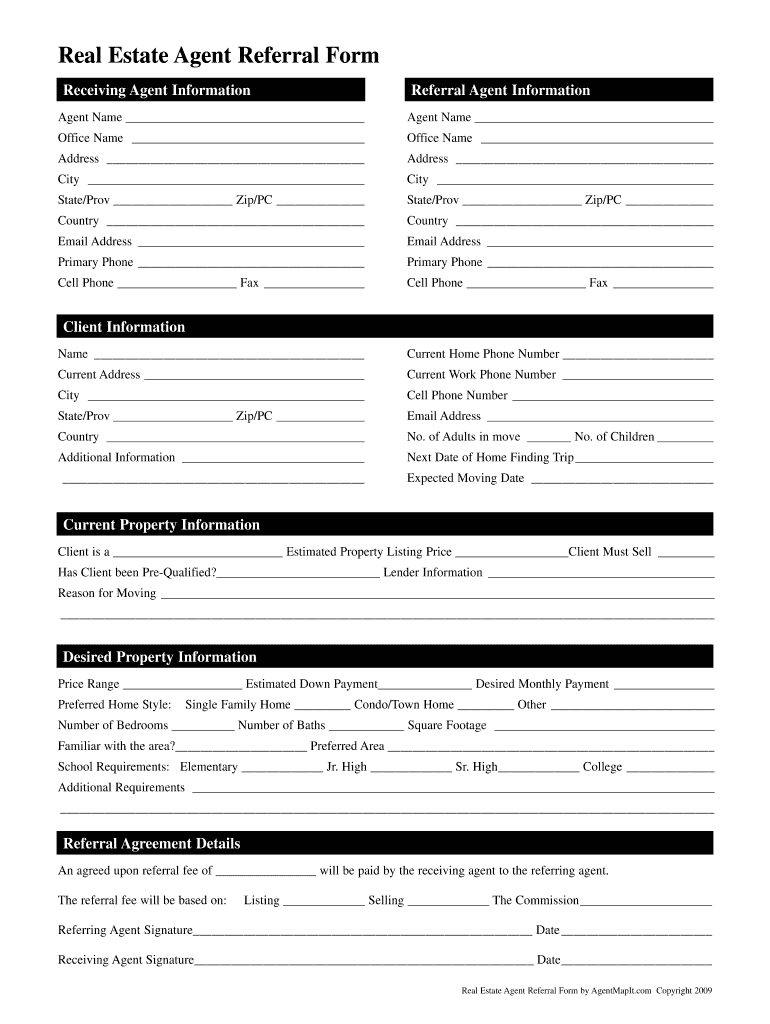
Referral Form Sample Download The Document Template
Request for external wheelchair assessment form. 2023 medicaid pa guide/request form (vendors). Cs day habilitation programs referral form. Web find helpful forms for molina healthcare members such as medical release forms, appeals request forms and more. 01/01/18) pregnancy notification form frequently used forms claims announcements.
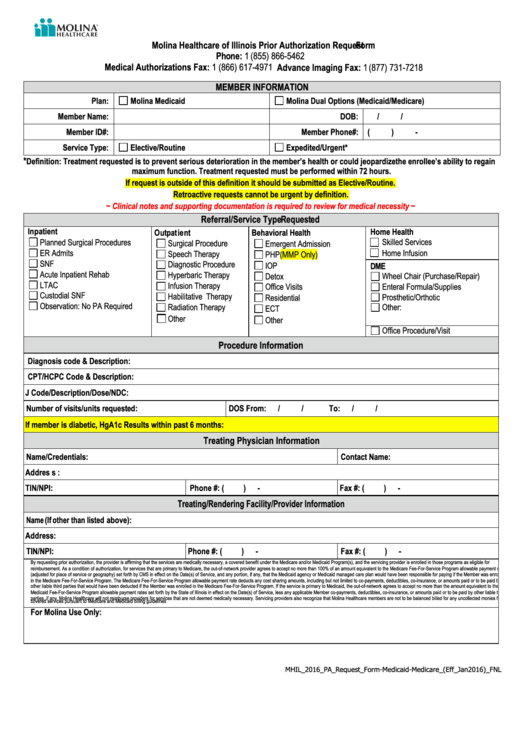
Molina Healthcare Of Illinois Prior Authorization Request printable pdf
2023 medicaid pa guide/request form (vendors). Web if you would like to appoint a representative, you and your appointed representative must complete this form and mail it to molina dual options at: Cs medically tailored meals referral form. Web molina healthcare of washington, inc. This referral is valid for 90 days or up to 6 months only.
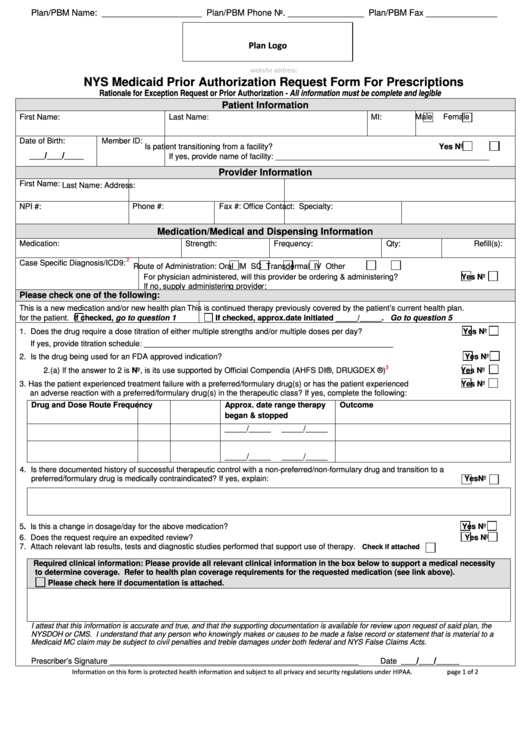
Fillable Nys Medicaid Prior Authorization Request Form For
Molina healthcare of california 200 oceangate, suite 100 long beach, ca 90802 01/01/18) pregnancy notification form frequently used forms claims announcements. Web critical incident referral template (medicaid only) ohio urine drug screen prior authorization (pa) request form. This referral is valid for 90 days or up to 6 months only. 2023 medicaid pa guide/request form (vendors).
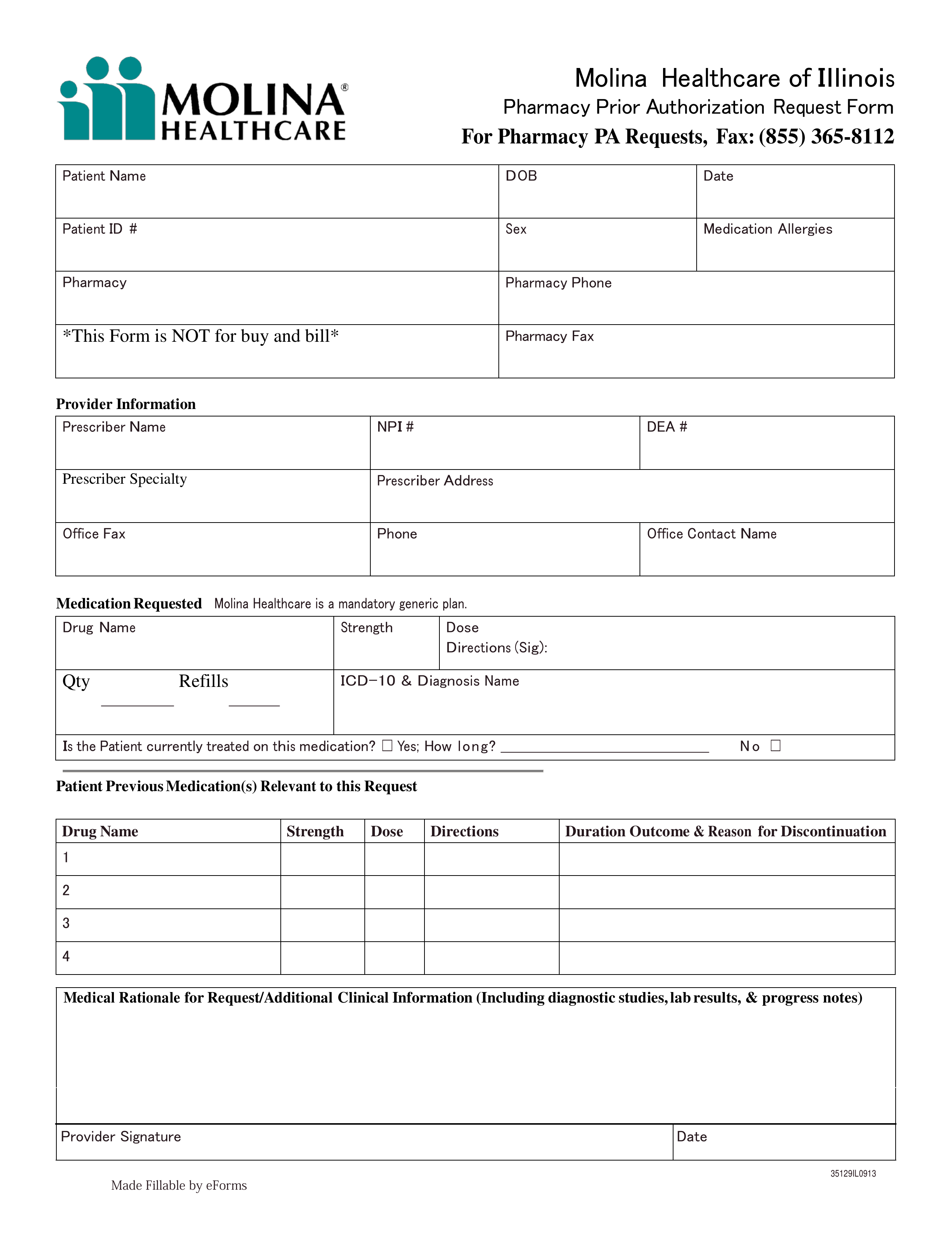
Free Molina Healthcare Prior (Rx) Authorization Form PDF eForms
This referral is valid for 90 days or up to 6 months only. Critical incident form email comped et l form o:t [email protected] type of incident (required by aso/mcos) ☐ severely adverse medical outcome or death occurring within 72 hours of transfer from a contracted behavioral facility to a medical treatment facility Referral or prior authorization is needed Molina healthcare.

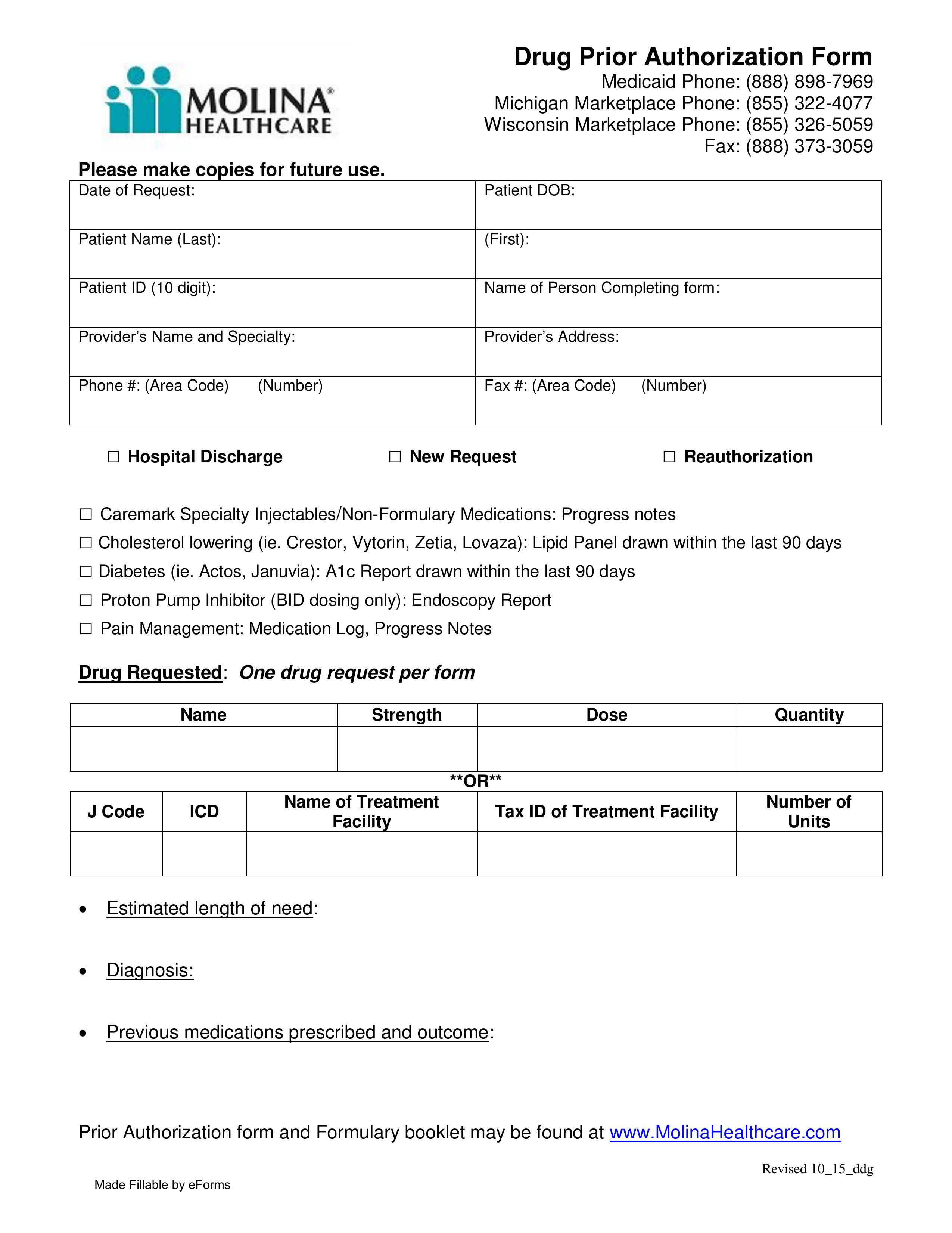
Molina Drug Prior Authorization Fill Online, Printable, Fillable
Cs recuperative care referral form. Request for external wheelchair assessment form. Web molina healthcare of washington, inc. 2023 medicaid pa guide/request form (vendors). Web if you would like to appoint a representative, you and your appointed representative must complete this form and mail it to molina dual options at:
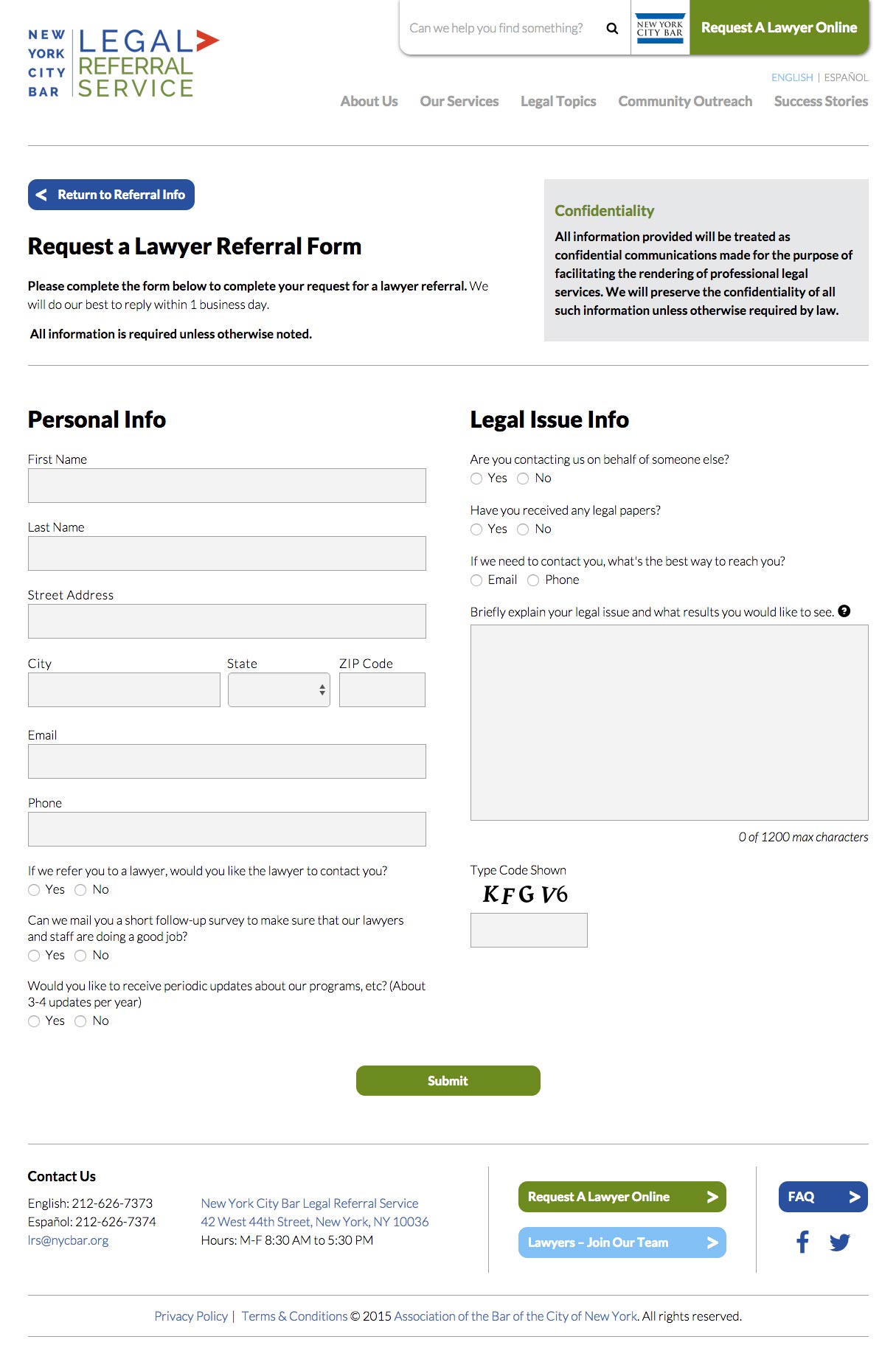
Harmonic Northwest » Blog Archive The AllNew NYC Legal Referral
Request for external wheelchair assessment form. Web if you would like to appoint a representative, you and your appointed representative must complete this form and mail it to molina dual options at: Web molina healthcare of washington, inc. Cs medically tailored meals referral form. Cs recuperative care referral form.
Free Molina Healthcare Prior (Rx) Authorization Form PDF eForms
Web find helpful forms for molina healthcare members such as medical release forms, appeals request forms and more. 01/01/18) pregnancy notification form frequently used forms claims announcements. Odm health insurance fact request form. Web molina healthcare of washington, inc. Cs medically tailored meals referral form.
Medicare Part D Medco Prior Authorization Form Printable
Request for external wheelchair assessment form. Cs day habilitation programs referral form. Odm health insurance fact request form. 2023 medicaid pa guide/request form (vendors). Web if you would like to appoint a representative, you and your appointed representative must complete this form and mail it to molina dual options at:
Referral Or Prior Authorization Is Needed
01/01/18) pregnancy notification form frequently used forms claims announcements. Cs day habilitation programs referral form. Critical incident form email comped et l form o:t [email protected] type of incident (required by aso/mcos) ☐ severely adverse medical outcome or death occurring within 72 hours of transfer from a contracted behavioral facility to a medical treatment facility Web if you would like to appoint a representative, you and your appointed representative must complete this form and mail it to molina dual options at:
Molina Healthcare Of California 200 Oceangate, Suite 100 Long Beach, Ca 90802
Cs personal care and homemaker services referral form. Web molina healthcare of washington, inc. Web find helpful forms for molina healthcare members such as medical release forms, appeals request forms and more. Cs recuperative care referral form.
Cs Medically Tailored Meals Referral Form.
2023 medicaid pa guide/request form (vendors). Odm health insurance fact request form. Request for external wheelchair assessment form. This referral is valid for 90 days or up to 6 months only.