Ohio Medicaid Sterilization Consent Form
Ohio Medicaid Sterilization Consent Form - You can also download it, export it or print it out. Web (1) claims for sterilization and hysterectomy procedures must be submitted to the department with either an original or a copy of the appropriate consent form. Web effective april 1, 2018, medicaid providers must submit odm 03199 “acknowledgement of hysterectomy information” and u.s. Statements are also included for an interpreter, a person obtaining consent, and a physician. Web ohio department of medicaid. Web this form allows an individual to provide consent for sterilization. Statements are also included for an interpreter, a person obtaining consent, and a physician. Web when submitting an abortion, sterilization, and/or hysterectomy procedure claim, please attach the appropriate consent form. Web send ohio medicaid sterilization consent via email, link, or fax. Edit, sign and save oh jfs 03198 form.
Web send ohio medicaid sterilization consent via email, link, or fax. Web when submitting an abortion, sterilization, and/or hysterectomy procedure claim, please attach the appropriate consent form. Web ohio department of medicaid. Download or email oh jfs 03198 & more fillable forms, register and subscribe now! Web this form allows an individual to provide consent for sterilization. Web sterilization consent form (age 21 and older) date (month/day/year) ohp 742a (7/16) statement of person obtaining consent Statements are also included for an interpreter, a person obtaining consent, and a physician. Web signature on this consent form and the date the sterilization procedure was performed. Web up to $40 cash back to comply with federal regulations, the ohio medicaid sterilization consent form must include the following information: (order form) healthchek & pregnancy related services information sheet.
You can also download it, export it or print it out. Web signature on this consent form and the date the sterilization procedure was performed. Healthchek & pregnancy related services information. Client medicaid or hhsc client number: Web effective april 1, 2018, medicaid providers must submit odm 03199 “acknowledgement of hysterectomy information” and u.s. Web up to $40 cash back to comply with federal regulations, the ohio medicaid sterilization consent form must include the following information: Statements are also included for an interpreter, a person obtaining consent, and a physician. Edit, sign and save oh jfs 03198 form. Web ohio department of medicaid. Download or email oh jfs 03198 & more fillable forms, register and subscribe now!

Medicaid Vasectomy Consent Form 2023 Printable Consent Form 2022
Web send ohio medicaid sterilization consent via email, link, or fax. Statements are also included for an interpreter, a person obtaining consent, and a physician. Download or email oh jfs 03198 & more fillable forms, register and subscribe now! Web up to $40 cash back to comply with federal regulations, the ohio medicaid sterilization consent form must include the following.

Ohio Medicaid Sterilization Consent Form 2022 Printable Consent Form 2022
Web other forms and resources. Ohio urine drug screen prior authorization (pa) request form. Date health insurance terminated per attached. Web signature on this consent form and the date the sterilization procedure was performed. Web if payment has been received from health insurance other than medicaid or medicare, please note first payment date.
Medicaid Sterilization Consent Form 2022 2022
Web ohio department of medicaid. (order form) application for health coverage & help paying costs. Application for health coverage & help paying price: Web this form allows an individual to provide consent for sterilization. Web (1) claims for sterilization and hysterectomy procedures must be submitted to odjfs the department with either an original or a copy of the appropriate consent.

Medicaid Appeal Form Ohio Form Resume Examples
Ohio urine drug screen prior authorization (pa) request form. Web this form allows an individual to provide consent for sterilization. Edit your medicaid consent for sterilization form ohio online. The consent for sterilization form. Web signature on this consent form and the date the sterilization procedure was performed.

Indiana Medicaid Sterilization Consent Form Instructions 2022
Your decision at any time not to be sterilized will not result in the withdrawal or. Application for health coverage & help paying price: Request for external wheelchair assessment form. (order form) healthchek & pregnancy related services information sheet. You can also download it, export it or print it out.
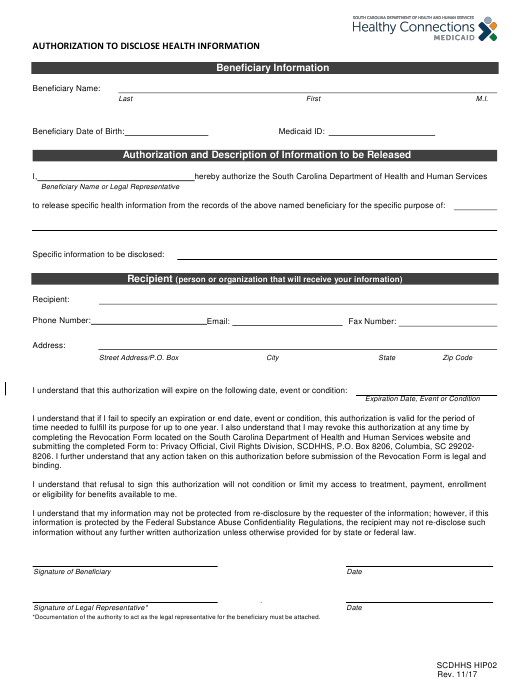
South Carolina Medicaid Sterilization Consent Form 2022 Printable
Edit your medicaid consent for sterilization form ohio online. Complete all fields unless indicated as optional. Web (1) claims for sterilization and hysterectomy procedures must be submitted to the department with either an original or a copy of the appropriate consent form. Statements are also included for an interpreter, a person obtaining consent, and a physician. Statements are also included.

Ohio Medicaid Sterilization Consent Form 2022 Printable Consent Form 2022
Web when submitting an abortion, sterilization, and/or hysterectomy procedure claim, please attach the appropriate consent form. Web (1) claims for sterilization and hysterectomy procedures must be submitted to odjfs the department with either an original or a copy of the appropriate consent form. Application for health coverage & help paying price: Web send ohio medicaid sterilization consent via email, link,.
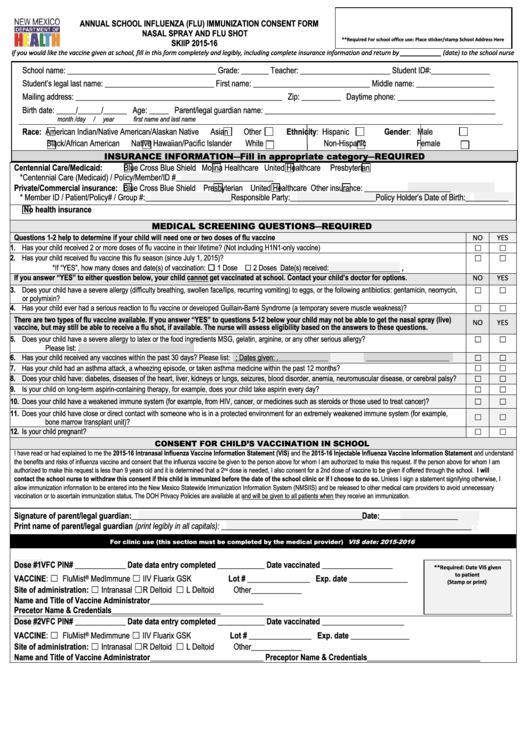
New Mexico Medicaid Sterilization Consent Form 2022 Printable Consent
Web signature on this consent form and the date the sterilization procedure was performed. Your decision at any time not to be sterilized will not result in the withdrawal or. Web the medicaid provider requesting payment for the sterilization submits to the department a copyof the consent form, completed in accordance with paragraph (b)(3). Download or email oh jfs 03198.

Don't the Consent Form on All Indiana Medicaid Sterilization
Client medicaid or hhsc client number: Download or email oh jfs 03198 & more fillable forms, register and subscribe now! Web signature on this consent form and the date the sterilization procedure was performed. Web when submitting an abortion, sterilization, and/or hysterectomy procedure claim, please attach the appropriate consent form. Complete all fields unless indicated as optional.
National Health Law Program Comments on Sterilization Consent Form
(order form) healthchek & pregnancy related services information sheet. Edit, sign and save oh jfs 03198 form. 72 hours after the date of the individual’s signature on this consent form because of the. Application for health coverage & help paying price: Web this form allows an individual to provide consent for sterilization.
Edit, Sign And Save Oh Jfs 03198 Form.
Web ohio department of medicaid acknowledgment of hysterectomy information name of patient's authorized representative (if any) instruction:. Web (1) claims for sterilization and hysterectomy procedures must be submitted to odjfs the department with either an original or a copy of the appropriate consent form. Web this form allows an individual to provide consent for sterilization. Download or email oh jfs 03198 & more fillable forms, register and subscribe now!
Web Sterilization Consent Form (Age 21 And Older) Date (Month/Day/Year) Ohp 742A (7/16) Statement Of Person Obtaining Consent
Web ohio department of medicaid. Complete all fields unless indicated as optional. (order form) healthchek & pregnancy related services information sheet. Ohio urine drug screen prior authorization (pa) request form.
Web Send Ohio Medicaid Sterilization Consent Via Email, Link, Or Fax.
Download or email oh jfs 03198 & more fillable forms, register and subscribe now! Web this form allows an individual to provide consent for sterilization. (order form) application for health coverage & help paying costs. You can also download it, export it or print it out.
Healthchek & Pregnancy Related Services Information.
Web if payment has been received from health insurance other than medicaid or medicare, please note first payment date. Identification of the individual giving. Statements are also included for an interpreter, a person obtaining consent, and a physician. Client medicaid or hhsc client number: