Optumrx Appeal Form Pdf
Optumrx Appeal Form Pdf - Web to submit a formal appeal, please see the instructions listed on the back of your explanation of payment (eop). Web health care provider application to appeal a claims determination submit to: Submissions with missing information will be invalid and excluded from. Web the advanced tools of the editor will lead you through the editable pdf template. Web up to 8% cash back appeal inappropriate medical necessity denials while also freeing resources on their internal appeals teams. Optumrx prior authorization guidelines the optumrx pharmacy. Az, ut, nv, co, nm, id, ks,. Claim information single multiple “like” claims (attach. Apply a check mark to indicate the choice. Web up to 8% cash back mac pricing appeal form date:
By supplying my credit card number, i authorize optum rx to maintain my credit card on file as payment method for any future charges. Find information on contracted provider reconsiderations, the appeals process, and the payment dispute process. Web • new users (to the optumrx provider portal) must create a new account. Web covered medication, and/or optumrx will offer information on the process to appeal the adverse decision. Web mac appeal form mac appeal detail must be filled out completely unless noted as optional. Web optumcare provider appeal unit p.o box 30539, salt lake city, ut 84130service phone: Apply a check mark to indicate the choice. Appeals must be submitted within 30 days or within such time period as may be required by applicable state. Web up to 8% cash back review and assess any denials. By monitoring a hospital’s claims and remittance.
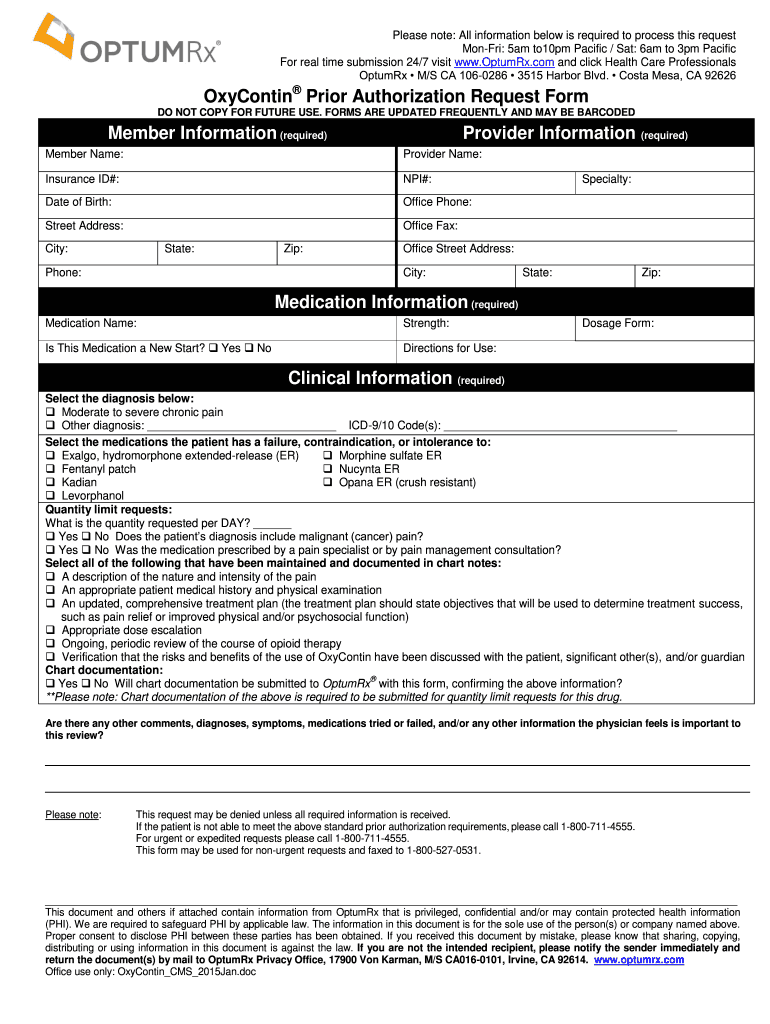
Apply a check mark to indicate the choice. Web have the right to ask us for a redetermination (appeal) of our decision. Optumrx prior authorization guidelines the optumrx pharmacy. Web member complaint and appeal form note: Add and replace text, insert new objects, rearrange pages, add watermarks and page numbers, and more. Az, ut, nv, co, nm, id, ks,. Enter your official contact and identification details. To obtain a review, submit a request in writing to the address below. Web covered medication, and/or optumrx will offer information on the process to appeal the adverse decision. Write customized appeal letters for insurance denial.
Optumrx Fax Number Form the Form in Seconds Fill Out and Sign
Web to submit a formal appeal, please see the instructions listed on the back of your explanation of payment (eop). Web expenses related to prescription orders. Web the advanced tools of the editor will lead you through the editable pdf template. By monitoring a hospital’s claims and remittance. By supplying my credit card number, i authorize optum rx to maintain.

Optumrx Medicare Part D Electronic Prior Authorization form Unique
Enter your official contact and identification details. Web to submit a formal appeal, please see the instructions listed on the back of your explanation of payment (eop). Web up to 8% cash back appeal inappropriate medical necessity denials while also freeing resources on their internal appeals teams. Get your fillable template and complete it online using the instructions provided. Add.
Optum rx oxycontin pa form Fill Out and Sign Printable PDF Template
Write customized appeal letters for insurance denial. Optumrx prior authorization guidelines the optumrx pharmacy. Apply a check mark to indicate the choice. By monitoring a hospital’s claims and remittance. Web up to 8% cash back appeal inappropriate medical necessity denials while also freeing resources on their internal appeals teams.
Optumrx Prior Authorization Form Cialis — Pharmacy General Exception Forms
• an account is required to submit a claim reimbursement review/ appeal request. Claim information single multiple “like” claims (attach. Web up to 8% cash back home. Web to submit a formal appeal, please see the instructions listed on the back of your explanation of payment (eop). Web have the right to ask us for a redetermination (appeal) of our.

Optumrx Medicare Part D Electronic Prior Authorization form Fresh
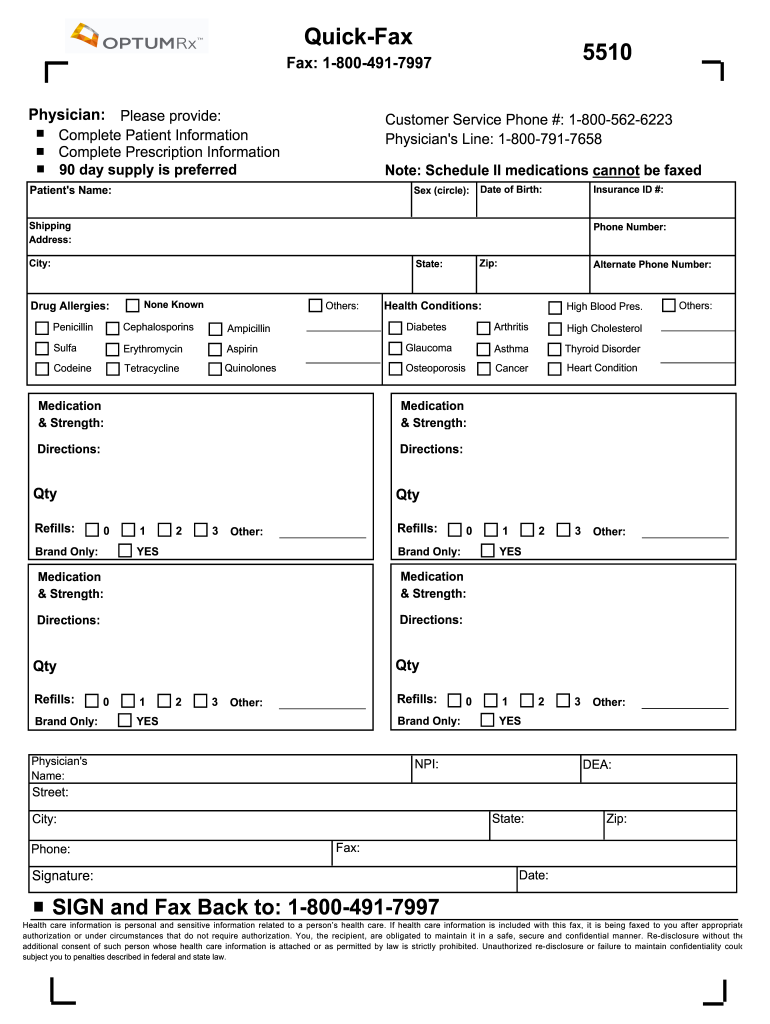
Web to submit a formal appeal, please see the instructions listed on the back of your explanation of payment (eop). Optumrx prior authorization guidelines the optumrx pharmacy. Web up to $40 cash back edit optumrx refill request form. Web covered medication, and/or optumrx will offer information on the process to appeal the adverse decision. Web mac appeal form mac appeal.
Optumrx Pharmacy Help Desk Sehbp Active Njea Member Prescription
Web have the right to ask us for a redetermination (appeal) of our decision. Claim information single multiple “like” claims (attach. Web up to 8% cash back appeal inappropriate medical necessity denials while also freeing resources on their internal appeals teams. Get your fillable template and complete it online using the instructions provided. Apply a check mark to indicate the.

Optumrx Medicare Part D Electronic Prior Authorization form
Berinert, cerezyme, cinryze, extavia, fabrazyme, kalbitor,. Web covered medication, and/or optumrx will offer information on the process to appeal the adverse decision. Web health care provider application to appeal a claims determination submit to: Web up to 8% cash back appeal inappropriate medical necessity denials while also freeing resources on their internal appeals teams. You have 60 days from the.
Free UnitedHealthcare Prior (Rx) Authorization Form PDF eForms
Find information on contracted provider reconsiderations, the appeals process, and the payment dispute process. Primary insured (transcribe as seen on your optumrx. • an account is required to submit a claim reimbursement review/ appeal request. Berinert, cerezyme, cinryze, extavia, fabrazyme, kalbitor,. Web have the right to ask us for a redetermination (appeal) of our decision.

OptumRx Medication Prior Authorization Request 2012 Fill and Sign
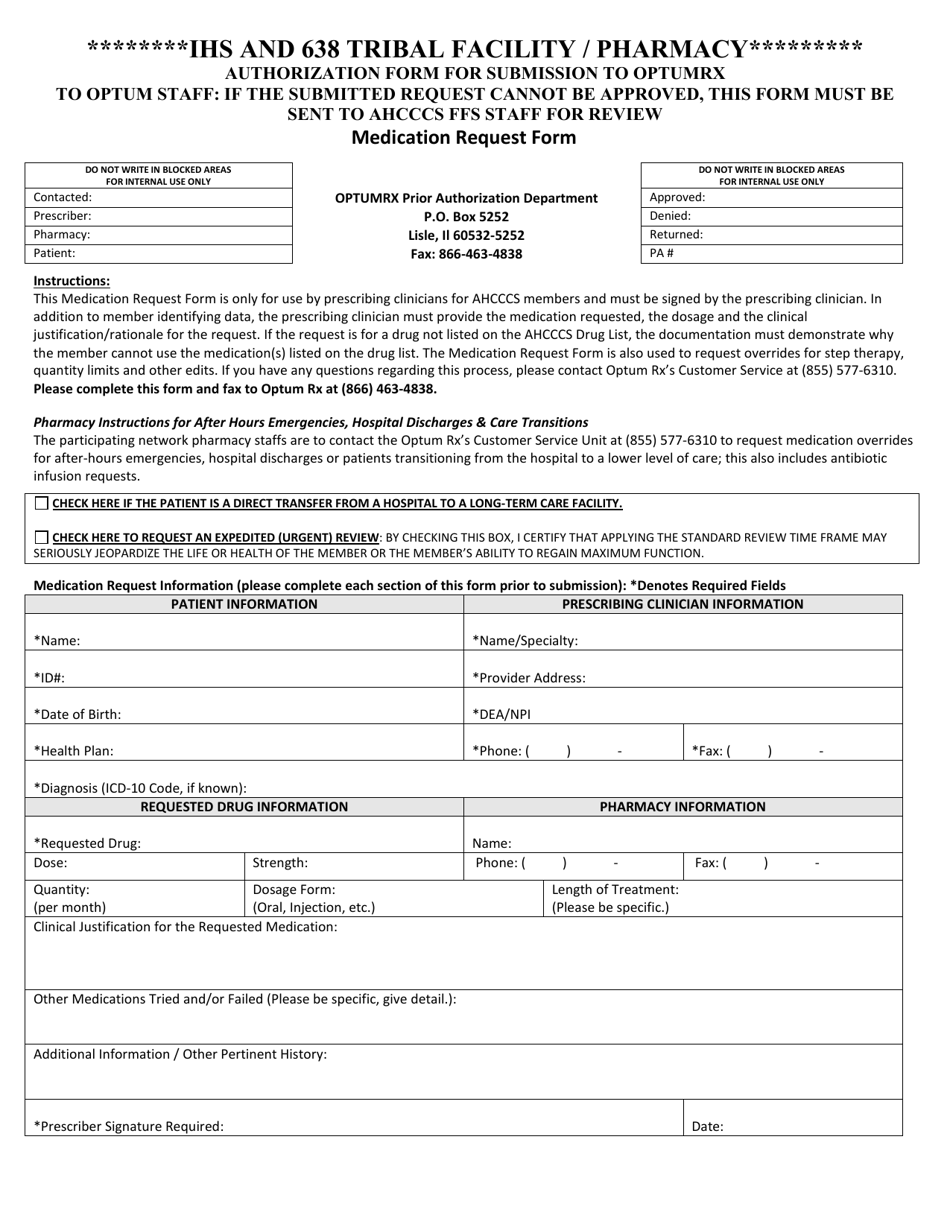
Web up to 8% cash back review and assess any denials. Web member complaint and appeal form note: Appeals must be submitted within 30 days or within such time period as may be required by applicable state. Claim information single multiple “like” claims (attach. You have 60 days from the date of our notice of denial of medicare prescription drug.

20132021 Form OPTUMRx 1040006 Fill Online, Printable, Fillable, Blank
Web have the right to ask us for a redetermination (appeal) of our decision. Az, ut, nv, co, nm, id, ks,. Submissions with missing information will be invalid and excluded from. Web expenses related to prescription orders. Web covered medication, and/or optumrx will offer information on the process to appeal the adverse decision.
Submissions With Missing Information Will Be Invalid And Excluded From.
Web up to 8% cash back mac pricing appeal form date: Web optumrx appeal form pdf. Berinert, cerezyme, cinryze, extavia, fabrazyme, kalbitor,. Apply a check mark to indicate the choice.
Write Customized Appeal Letters For Insurance Denial.
Web up to $40 cash back edit optumrx refill request form. Web health care provider application to appeal a claims determination submit to: Enter your official contact and identification details. Web expenses related to prescription orders.
Claim Information Single Multiple “Like” Claims (Attach.
By monitoring a hospital’s claims and remittance. Web optumcare provider appeal unit p.o box 30539, salt lake city, ut 84130service phone: Appeals must be submitted within 30 days or within such time period as may be required by applicable state. Web covered medication, and/or optumrx will offer information on the process to appeal the adverse decision.
Add And Replace Text, Insert New Objects, Rearrange Pages, Add Watermarks And Page Numbers, And More.
Web the advanced tools of the editor will lead you through the editable pdf template. Web up to 8% cash back review and assess any denials. Web up to 8% cash back home. Find information on contracted provider reconsiderations, the appeals process, and the payment dispute process.