Xolair Enrollment Form Pdf
Xolair Enrollment Form Pdf - Moderate to severe persistent asthma in adults and pediatric patients 6 years of age and older with a positive skin test or in vitro. Web prescription & enrollment form: Blue cross and blue shield of texas. Web find xolair® (omalizumab) support for our practice, including financial supports, billing and distribution information, office support materials, & patient education resources. Web 1 of 2 prescription & enrollment form: Web please print and complete the forms below. Referral forms for xolair® (omalizumab): (a) patient has been established on therapy with xolair for moderate to severe persistent. Middle initial date of birth prescriber’s. Web xolair will be approved based on one of the following criteria:
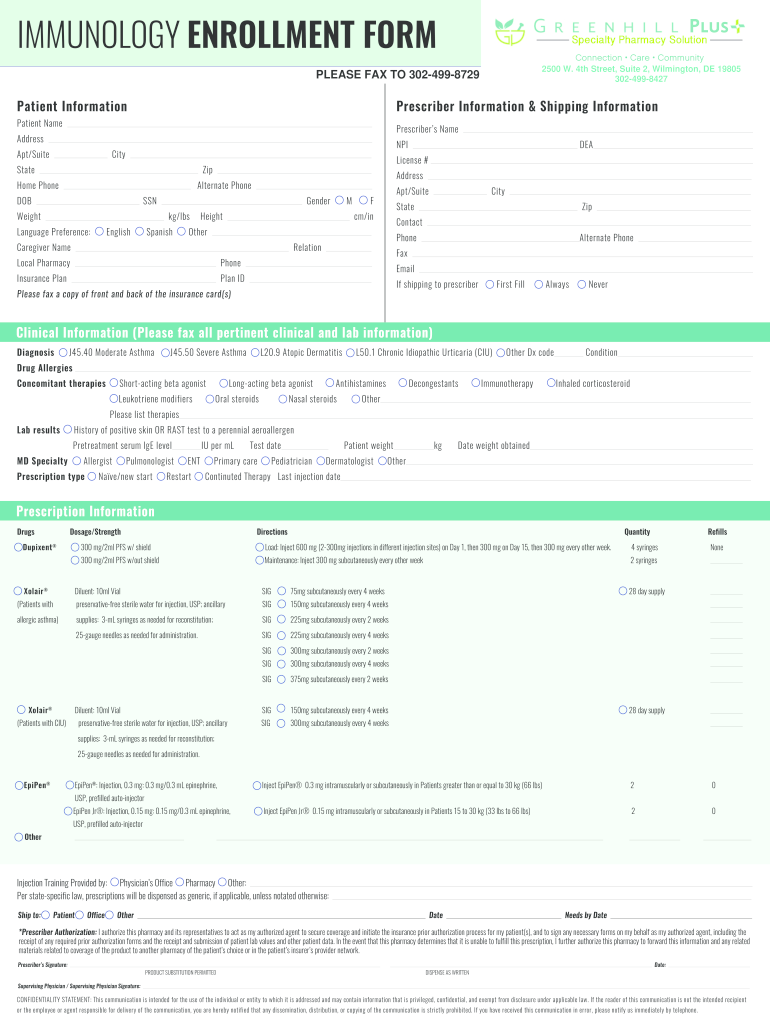
Web xolair® (omalizumab) enrollment form xolair® (omalizumab) enrollment form fax completed form to: Web download the form you need to enroll in genentech access solutions. Middle initial date of birth prescriber’s. Web xolair ® (omalizumab) prescription type: Xolair ® (omalizumab) fax completed form to 866.531.1025. Referral forms for xolair® (omalizumab): These instructions are to be used for both dose strengths. Web step 14 “after the injection”) xolair prefilled syringes are available in 2 dose strengths. 150 mg/dose subcutaneously every 4 weeks 300 mg/dose subcutaneously. Use this form to enroll patients in xolair.
Web step 14 “after the injection”) xolair prefilled syringes are available in 2 dose strengths. Web patient enrollment and consent form for patients prescribed prxolair® for moderate to severe allergic asthma (aa), chronic idiopathic urticaria (ciu), or severe chronic. These instructions are to be used for both dose strengths. Once completed, fax to the number indicated on the form. 150 mg/dose subcutaneously every 4 weeks 300 mg/dose subcutaneously. Xolair® (omalizumab) fax completed form to 808.650.6487. Web both the prescriber service form and the patient consent form must be received before xolair access solutions can begin helping your patient. Web the xolair recertification reminder program helps eligible patients avoid potential gaps in their xolair therapy due to insurance recertification requirements. Web prescription & enrollment form: Web xolair will be approved based on one of the following criteria:
Xolair Enrollment Form Enrollment Form
Web prescription & enrollment form: Middle initial date of birth prescriber’s. Web xolair ® (omalizumab) prescription type: Web download the form you need to enroll in genentech access solutions. Web xolair will be approved based on one of the following criteria:

XOLAIR® (omalizumab) Injection Preparation and Administration
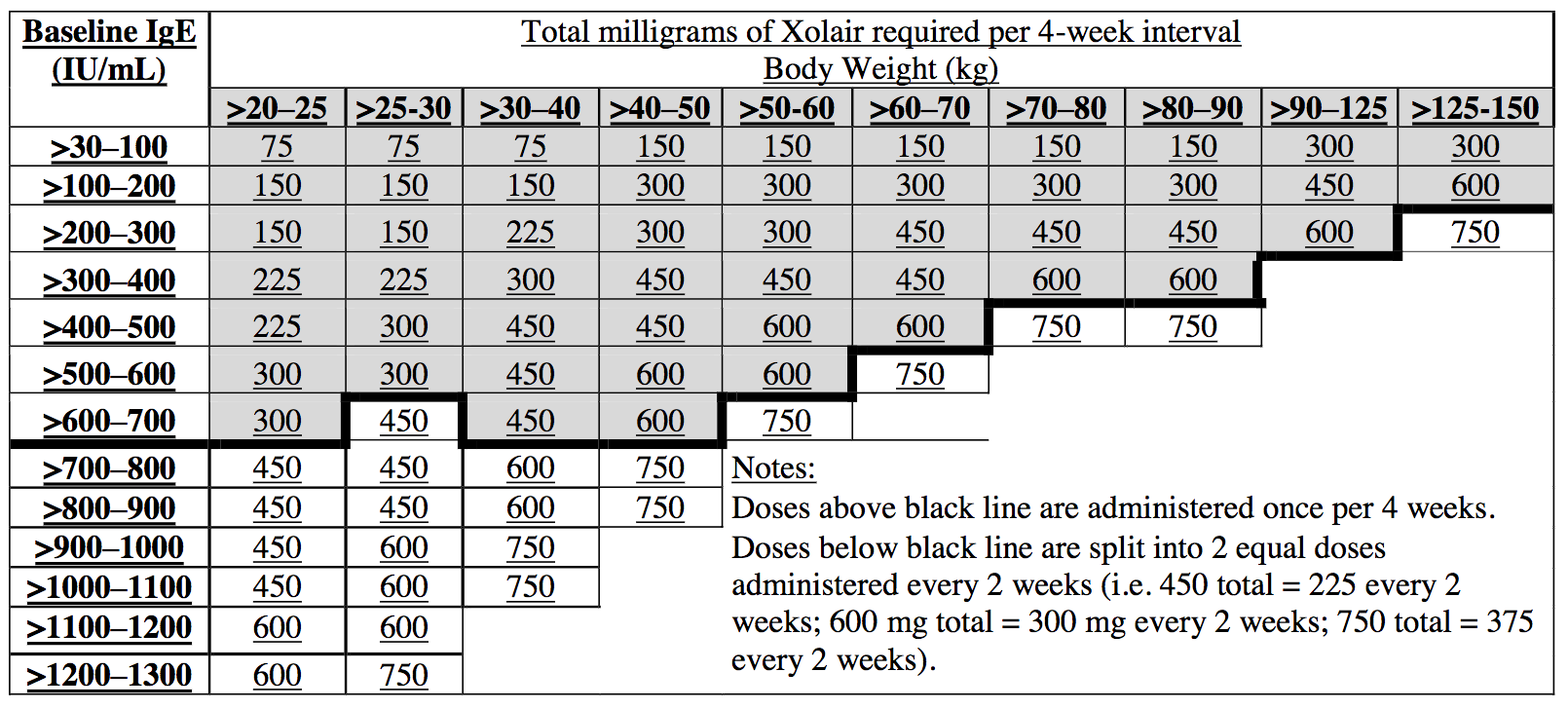
Referral forms for xolair® (omalizumab): Web 4 prescribing information medication strength/formulation directions quantity/refills xolair® (omalizumab) asthma(dose is dependent on weight and ige. (a) patient has been established on therapy with xolair for moderate to severe persistent. Web please print and complete the forms below. Patient’s first name last name middle initial date of birth prescriber’s first.
Xolair requirement Centre of Excellence in Severe Asthma
Xolair ® (omalizumab) fax completed form to 866.531.1025. Web patient enrollment and consent form for patients prescribed prxolair® for moderate to severe allergic asthma (aa), chronic idiopathic urticaria (ciu), or severe chronic. Web the xolair recertification reminder program helps eligible patients avoid potential gaps in their xolair therapy due to insurance recertification requirements. Use this form to enroll patients in.
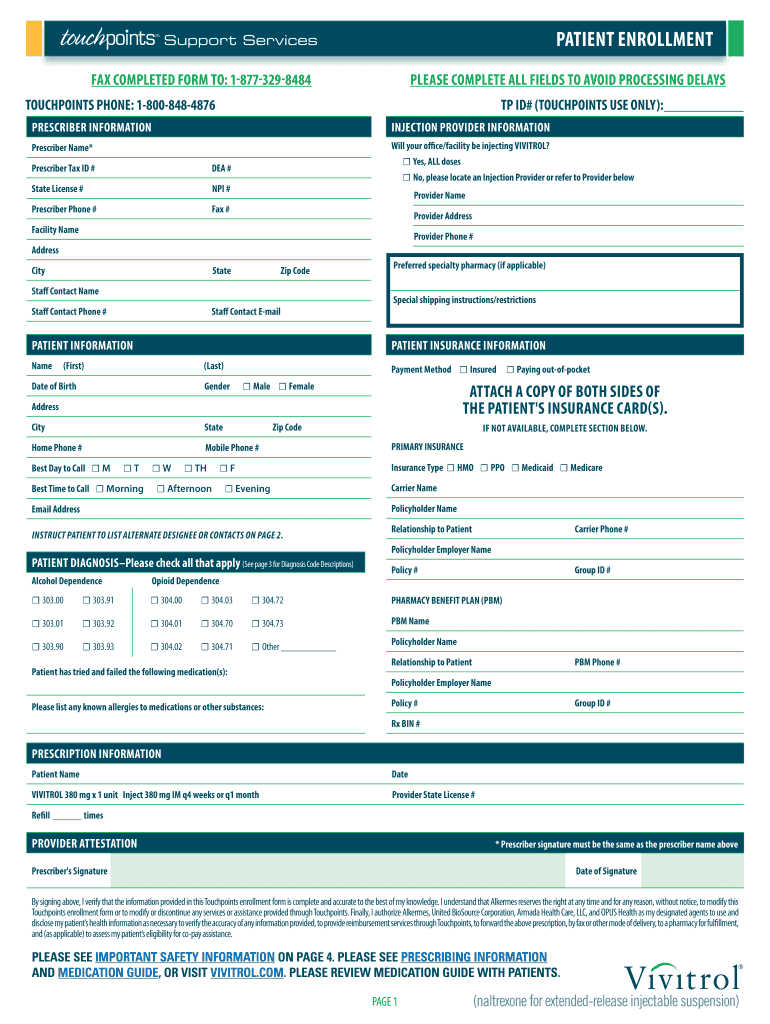
Vivitrol Enrollment Form Fill Out and Sign Printable PDF Template
Moderate to severe persistent asthma in adults and pediatric patients 6 years of age and older with a positive skin test or in vitro. Middle initial date of birth prescriber’s. Naïve/new start restart continued therapy. Once completed, fax to the number indicated on the form. Web xolair enrollment form date:
![29 [PDF] XOLAIR APPROVAL FORM FREE PRINTABLE DOCX 2020 ApprovalForm2](https://data.formsbank.com/pdf_docs_html/123/1235/123591/page_1_thumb_big.png)
29 [PDF] XOLAIR APPROVAL FORM FREE PRINTABLE DOCX 2020 ApprovalForm2
Web download the form you need to enroll in genentech access solutions. Twelvestone health partners fax referral to: Web 1 of 2 prescription & enrollment form: Web xolair ® (omalizumab) prescription type: Web step 14 “after the injection”) xolair prefilled syringes are available in 2 dose strengths.

SchoolEnrollmentForm.pdf DocDroid
Xolair® (omalizumab) fax completed form to 808.650.6487. Start enrollment with the patient consent form to get started, fill out the patient consent form. Web the xolair recertification reminder program helps eligible patients avoid potential gaps in their xolair therapy due to insurance recertification requirements. Web find xolair® (omalizumab) support for our practice, including financial supports, billing and distribution information, office.
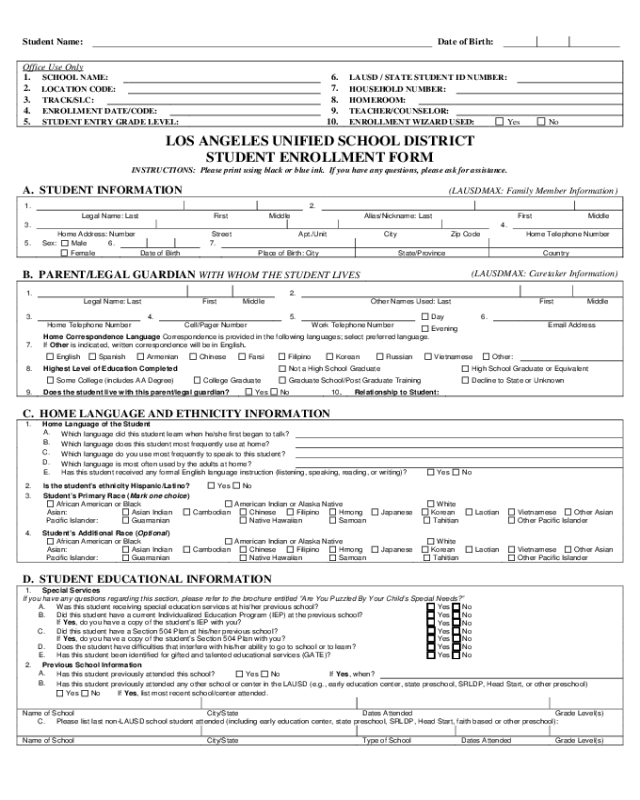
Student Enrollment Form California Edit, Fill, Sign Online Handypdf
Start enrollment with the patient consent form to get started, fill out the patient consent form. Moderate to severe persistent asthma in adults and pediatric patients 6 years of age and older with a positive skin test or in vitro. Web xolair® (omalizumab) enrollment form xolair® (omalizumab) enrollment form fax completed form to: Web xolair ® (omalizumab) prescription type: Twelvestone.

Sample Ach Enrollment Form Form Resume Examples goVLPd3Vva
150 mg/dose subcutaneously every 4 weeks 300 mg/dose subcutaneously. Web find xolair® (omalizumab) support for our practice, including financial supports, billing and distribution information, office support materials, & patient education resources. Web xolair ® (omalizumab) prescription type: Web step 14 “after the injection”) xolair prefilled syringes are available in 2 dose strengths. Web patient enrollment and consent form for patients.

XOLAIR Dosage & Rx Info Uses, Side Effects The Clinical Advisor
Web patient enrollment and consent form for patients prescribed prxolair® for chronic idiopathic urticaria (ciu), all sections must be completely filled out (please print). Middle initial date of birth prescriber’s. Once completed, fax to the number indicated on the form. Xolair® (omalizumab) fax completed form to 808.650.6487. Web xolair® (omalizumab) enrollment form xolair® (omalizumab) enrollment form fax completed form to:
MS Enrollment Form PDF Host
Web xolair will be approved based on one of the following criteria: Middle initial date of birth prescriber’s. Web please complete the form below to join support for you. Web xolair prior authorization request form please complete this entire form and fax it to: These instructions are to be used for both dose strengths.
(1) All Of The Following:
Web xolair ® (omalizumab) prescription type: Web xolair will be approved based on one of the following criteria: Start enrollment with the patient consent form to get started, fill out the patient consent form. Twelvestone health partners fax referral to:
Blue Cross And Blue Shield Of Texas.
Web xolair® (omalizumab) enrollment form xolair® (omalizumab) enrollment form fax completed form to: Web download the form you need to enroll in genentech access solutions. 150 mg/dose subcutaneously every 4 weeks 300 mg/dose subcutaneously. Web please complete the form below to join support for you.
Before Providing Your Information, Let’s Confirm That You Are Eligible To Join Today.
Moderate to severe persistent asthma in adults and pediatric patients 6 years of age and older with a positive skin test or in vitro. Patient’s first name last name middle initial date of birth prescriber’s first. Use this form to enroll patients in xolair. These instructions are to be used for both dose strengths.
Web Xolair Prior Authorization Request Form Please Complete This Entire Form And Fax It To:
Referral forms for xolair® (omalizumab): Web step 14 “after the injection”) xolair prefilled syringes are available in 2 dose strengths. Web find xolair® (omalizumab) support for our practice, including financial supports, billing and distribution information, office support materials, & patient education resources. Xolair ® (omalizumab) fax completed form to 866.531.1025.